PARS OFFICIALIS
Date: 2015-10-07; view: 555.
Curator: Alzawahreh Mohammed
Patient: AndriyVolodymirovychBoycan
TOPIC 15: Modern system of international relations
This lecture focuses on modern system of international relations and the role of the USA in the international relations. We also examine the role of the multilateral organizations such as the United Nations in providing international peace of security with the special focus on the UN Security Council. Role of NATO in the post-Cold War period is also discussed.
3rd course, 57+ group of General Medicine faculty.
• PASSPORT DATA AND GENERAL INFORMATIONS –
• AndriyVolodymirovychBoycan
• 24 years old
• Male
• Position - Student
• Date of admission – 18.04.2014
• Sent by GP
• Diagnosis at admission – Bronchial Asthma
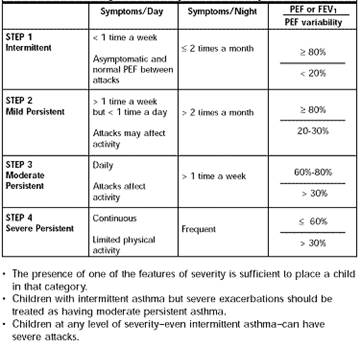
• Clinical diagnosis – Bronchial Asthma second stage, moderate exacerbation, pulmonary insufficiency of first degree.
• PATIENT COMPLAINTS – MOLESTIAE AEGROTI
• Dyspnea in expiration, whistling respiration, dry paroxysmal nocturnal cough with sputum.
• MEDICAL HISTORY OF THE BODY SYSTEMS – ANAMNESIS COMMUNIS
Respiratory system:
• Cough – Dry, paroxysmal nocturnal cough with transparent sputum. Intermediate duration. Couple of times during the night. Moderate severity.
• Sputum – transparent, glassy sputum. Odorless, easy discharge with cough.
• Hemoptysis absent.
• Chest pain – absent
• Shortness of breath – Expiratory dyspnea. Paroxysmal attacks mainly during the nighttime. Moderate duration and intensity. Also dyspnea intensifies after exercises and passes through during the rest.
• The best position during the attack is with hands well situated on the wall or on the table.
• Wheezing expiration.
• Tachypnea – in acute attack – to 25/min.
Cardio-vascular system:
• Pain in precordial area is absent, no disruption of the heart.
• Heartbeat around 100 bpm – tachycardia.
• No edema.
• No headaches, no “dead fingers”, no limb swelling and no pain.
The Digestive system:
• No pain and no other discomfort. A small obesity is present.
• Appetite – very good.
• Thirst – in normal
• Heartburn sometimes present – reflux.
• No nausea, no vomiting present, Salivation and chewing in normal.
• Defecation regular, up to 2/day.
• Stool normal, brown, with normal smell, no worms or artificial contaminants.
• Gases discharge – free, communicated with food.
Urinary system:
• No pain.
• Urination normal, regular.
• Urination mostly during the day – seldom at night.
• No artificial contaminants.
• Urine – light yellow, normal smell, clear.
Locomotion system:
• Pain absent. Sometimes dull pain in the chest muscles – very seldom after an acute attack.
• No other complaints.
Endocrine system:
• Skin dry, during attack acrocyanosis appears.
• Body weight – 98kg, height 179cm – small obesity.
Nervous system and sense organs:
• No complaints
• No headache, no dizziness.
Bloodsystem:
• No bone pain.
• No hemorrhages.
• No other complaints.
• GENERAL COMPLAINTS – MOLESTIAE COMMUNIS
• Fever absent.
• Chills sometimes appear after the acute attack.
• Sweating appears during the attack.
• Malaise, weakness and fatigue present and common.
• ANAMNESIS MORBI
• First symptoms appeared about 2 years ago after physical exercises.
• The beginning of the symptoms were acute, but in the beginning the attacks were not so strong as they are now. The attacks have been appearing more seldom than now. At the beginning the attack were appearing about 1 time a week and acute phase were very short. Now the attacks are more frequent – more than 2 times a week but not more than 1 time a day. The acute attacks interfere with dream during the night and with daily activity. The nocturnal attacks appear more than 2 times in a month.
• The exacerbation increases after physical exercises or during cold days. Often appear in case of dust inhalation or in case of emotional stress.
• First manifestation in hospital appeared a day after the admission on 19.04.2013. It has been an acute attack during the nighttime.
• Deterioration appears during night and after exercises. Facilitation at rest and in position which involves all muscles helping in breathing.
• Exacerbation appears during cold days, breathing in dusty environment and after exercises.
• Relapses – more than 2 times a week of acute attacks, but still <1/day.
• Treatment till now has been against infections of upper respiratory tract.
• Present manifestation – dyspnea, weakness, fatigue. Acute manifestation – sharp attack of dyspnea, tachypnea, tachycardia, expiratory wheezing and crackles.
• HISTORY OF LIFE – ANAMNESIS VITAE
• Patient born in Ivano-Frankivsk in 10.01.1989
• Grew up in the flat with parents and 2 sisters. The patient hasn't had any problems with learning and friendships during the childhood and adolescence.
• The patient smokes cigarettes for over 8 years – now up to 2 packs a day.
• The patient has been working in a restaurant for smokers for 2 years.
• Now the patient is studying on the University of Oil and Gas in Ivano-Frankivsk.
• During the weekends patient is meeting his friends and they spend the time in bars.
Conditions:
• The patient still lives with his parents and one sister. The other sister moved to her own flat.
• The family of the patient is the middle wealthy and have no financial problems.
• The patient likes to eat much pork meat, fat and he doesn't eat regularly.
• Now he keeps staying in the fresh-air places, but during the weekends he spends time in smokers clubs.
• The patient doesn't do any exercises, because it cause acute attacks of dyspnea and cough.
• The patient smokes cigarettes – up to 40 pieces per day. During the night about 2-3 pieces. He also drinks alcohol from time to time. Doesn't take narcotics.
• The patient has very wide history of diseases of upper respiratory tract which were sometimes transported on the lungs causing bronchitis and pneumonias.
• The patient has been ill to Pneumonia 2 times in his lifetime. First time when he was 8 years old, second time when he was 20 years old. Twice hospitalized. Tuberculosis and hepatitis were absent. AIDS not present.
• One wound of a forearm is present caused by car accident.
• The patient's mother and grandmother have problems with cardio-vascular system – Arterial hypertension. Father has Diabetes Mellitus Type 2.
Allergic history:
• Attacks of sneezing appear in dusty environment.
• Physical activity causes acute attacks of cough and dyspnea.
• No other allergic reactions to medicines, weather, food, smells, or insect bites.
Professional history:
• The patient has been working in a restaurant for 2 years. After that he became a student in University of Oil and Gas in Ivano-Frankivsk.
• Regular holidays the patient spends in the city.
• Studies take from 6 to 8 hours a day.
Epidemiological history:
• The patient hasn't had contact with patients with infectious diseases in past years.
• He hasn't had any insect bites that he remembers.
• INSPECTIO COMMUNIS
• The general condition of the patient is moderate. He is fatigued and weakened.
• State of mind – clear with no noticeable disorders.
• The position in the bed is active, but during the acute attack – passive.
• The posture – correct.
• Facial expression – normal. During the attack acrocyanosis appears.
• Skin – pale pink, but during the attack the skin on fingers, nose, lips become bluish. Skin is a little bit dry, good flexibility.
• Hair – dark brown, in normal.
• The nails –Clubbed
• No ulcers and rashes in mucous membranes.
• Subcutaneous fat well distributed on the abdomen mainly.
• No swelling.
• Lymph nodes not enlarged, soft, movable, regular shape not painful.
• Muscles normally developed, with normal strength and tone. After an acute attack some tremor appears.
• The chest hyperinflated. No other deformations.
• Joints in good condition. Movements normal, not painful.
• Respiration mixed type. Both halves of the thorax act in respiration. During palpation voice trembling weakened. In comparative percussion the sound is hyper sonorous, diaphragmatic depression and lowering of the lung borders.
• During auscultation may be heard both-sided wheezing and crackles. Extended expiration, tachycardia and tachypnea, stridor.
• The HB equal to 100 bpm, rhythm regular and normal intensity. The BP is 100/70. During auscultation of the heart the apex found in anatomical position. The cardiac borders anatomically normal. Cardiac sounds clear, no murmurs present.
• GIT in normal. Abdomen spherical. Anterior wall participate in respiration.
• The rectum and anus without visible hemorrhoid nodes, no fistulas and fissures.
• The urinary system in normal.
• The nervous system –all in normal.
• INITIAL DIAGNOSIS – DIAGNOSIS PRUELIMINARIS
• Bronchial asthma.
• Patient has been using self-treatment with analgesics and inhalations.
• PLAN OF EXAMINATION
• General blood test – Leucocytosis and eosinophilia.
• Test for IgE-dependent allergy – negative
• Spirometry – FEV1 = 80% - better after inhalation of B2-mimetics.
• PEF for 2-4 weeks – daily changes between 20% and 30%.
• Chest X-RAY – Hyperinflation.
• Pulsoxymetry and gazometry of arterial blood – PaO2 increased, PaCO2 decreased – hyperventilation.
• Test of concentration of NO in expiration.
• Sputum culture test.
• INSTRUMENTAL EXAMINATION
• Bronchoscopy, bronchography – Bronchial obstruction.
• CLINICAL DIAGNOSIS – DIAGNOSIS CLINICA
• Bronchial Asthma of second stage, moderate exacerbation with pulmonary insufficiency of Ist degree after the algorhytm:
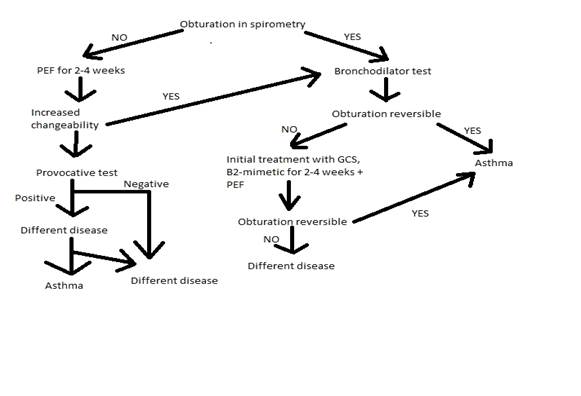
• Classification of asthma:
• 
• TREATMENT
• Treatment according to severity:

• Patient has 2nd stage asthma so the treatment will involve GCS and B2-mimetics such as Salbutamol or Ventolin.
• PROGNOSIS
• Patient is supposed to take the medicines for the rest of his life. Life-threating attacks may occur if the asthma will not be properly cured. The physical work and exercises are not recommended in extense.
| <== previous lecture | | | next lecture ==> |
| | | Цели и задачи дисциплины. |